Big Change
My own journey on the importance of early childhood started with adults, not children...
When first undertaking royal duties a decade ago, I started meeting inspiring people who were rebuilding their lives from challenges such as addiction, homelessness, violence — and the mental ill health that often underpins these experiences. Spending time together and hearing more about their lives, I was struck by how often poor mental health but also early childhood was the focus of our conversation.
It was the recurrence of these conversations that drove me to want to learn more. And I am indebted to the academics, practitioners and, of course, parents who shared their knowledge so generously with me. Because by understanding the data, observing the practice and listening to lived experience, it became clear that if we want to build a happier and mentally healthier society then one of the best investments we can make is in the relationships, environments and experiences that make up our early childhoods.
What this report makes clear is that our first five years lay important foundations for our future selves. This period is when we first learn to manage our emotions and impulses, to care and to empathise, and thus ultimately to establish healthy relationships with ourselves and others.
It is a time when our experience of the world around us, and the way that this moulds our development, can have a lifelong impact on our future mental and physical wellbeing. Indeed, what shapes our childhood shapes the adults and the parents we become. But — and this is crucial to understand — even if we ourselves didn’t get the best start in life we can still break the cycle and develop the skills needed to raise the next generation better.
What this means is that we need to go beyond physical needs and give focus to social and emotional needs too. Nurtured children are the consequence of nurturing adults. So to invest in children means also investing in the people around them — the parents, carers, grandparents, early years workforce and more. And therefore, transforming early childhood comes back to each and every one of us. There are so many ways in which we can all support, whether as private, public and voluntary sectors, as individuals or as communities. Investing in a child is ultimately an investment in our future societal health and happiness, but to achieve this vision we need the whole of society to play its part.
In establishing The Royal Foundation Centre for Early Childhood, our mission is to drive awareness of, and action on, the transformative impact of the early years. We aim to change the way people think about early childhood — and this report is our first step. We will help to make change through fresh research to identify opportunities, collaborations to scale solutions and creative campaigns to bring this issue to life.
We will do this by continuing to listen to others and being informed by the data.
I hope this report inspires you to join this journey.
It won’t be easy — transformation never is — but big change starts small.
Executive summary
Early childhood represents one of the best investments we can make for the long-term health, wellbeing and happiness of our society. Our future outcomes, whether they be academic, economic or health-related (including mental health), are profoundly shaped by our first five years. Yet The Royal Foundation’s landmark public survey on early childhood, conducted by Ipsos MORI in 2020, revealed that recognition of the importance of the early years is low.
This report is published to coincide with the launch of The Royal Foundation Centre for Early Childhood. It is a summary of decades of science on early childhood and research on why the early years matter. By bringing this body of evidence together, we hope to demonstrate the strategic importance of this vital issue to everybody. Just as decades of climate science breakthroughs have shown a path towards a more sustainable future, so too can these insights demonstrate the power of early childhood in building strong, healthy societies. That is the purpose of this report and the underlying strategic thought of The Royal Foundation Centre for Early Childhood.
This report also aims to show unequivocally that, by working together, there are real opportunities for us all — as caregivers, professionals, communities, businesses and society more widely — to prioritise the early years and to change the way we think about early childhood development. And it is in our common interests to do so. Providing as much protection as we can in the early years (from pregnancy through to the age of five) is our best opportunity to address today’s mental health crisis and to secure our long-term health and wellbeing.
In the first chapter, ‘Shaping Our Lives’, we set out in summary the science of early childhood development and explain why healthy brain development is vital in the first five years. With expertise from The Center on the Developing Child at Harvard University and from neuroscientists and academics in the UK who are part of our steering group, we explain why the early years offer such a huge opportunity to lay the foundations for healthy development, with potential life-long benefits for mental and physical health. Indeed, a clear association has been found between early childhood experiences and life outcomes, including financial wellbeing and factors such as addiction and crime.
Crucially, the science tells us that while genes play a huge role, development is not pre-determined. From pregnancy onwards, the context in which we develop matters too. Supporting healthy development in early childhood goes far beyond looking after the physical needs of babies and infants. Our earliest relationships, environments and experiences can profoundly shape the developing brain, which is characterised by exceptional plasticity during this period. This in turn influences the adults we become and also how we parent the next generation.
All those helping to raise children are key to nurturing healthy development and building resilience. Simple, consistent and responsive interactions between caregiver and child strengthen neural connections in the brain and contribute to secure attachment — a sense of safety and security, help with regulating emotions and a safe base from which to explore. These early stages of development, and the brain circuits that underpin them, are all formed in the earliest years. They help infants learn how to regulate their emotions, feelings and behaviour, and build their sense of agency and confidence to ultimately navigate their physical and social worlds independently.
This means that all those raising our under-fives themselves need both practical and emotional supports. A caregiver’s ability to support a child depends on their own wellbeing and mental health, and their understanding of their own emotions and the feelings of others around them.
The second chapter, ‘The Economics of the Early Years’, looks at the financial costs to society of failing to make the most of the golden opportunity of the early years. The Royal Foundation has partnered with the London School of Economics to calculate the cost of lost opportunity in early childhood, and has found that in England alone we are paying at least £16.13 billion each year. This is the cost to society of the remedial steps we take to address issues — from children in care to short- and long-term mental and physical health issues — that might have been avoided through action in early childhood. This sum of £16.13 billion is equivalent to nearly five times the total annual spend in England on early education and childcare entitlements, and around 44 times the annual expenditure on specialist perinatal mental health support.
While a figure of £16.13 billion sounds high, it is in reality an underestimate, excluding for example the later costs of unmet need and the knock-on impacts for other individuals and relationships which may be harmed as a consequence of failing to provide the right support early on. It also says nothing of the losses to the productivity and earnings of individuals over their lifetime — which in US studies have been shown to be sizeable.
This new estimate points to the huge opportunity created by investment in early childhood. Economic evidence is growing all the time about ‘what works’ — both in terms of individual early years programmes and whole system changes — to provide effective and preventative early help rather than later, remedial support. And there is a growing consensus across communities, sectors and traditional political divides on tackling this imbalance in years to come.
In the third chapter, ‘Where We Are Now’, we ask how babies, young children and their families are doing in the UK today and explore the strength of the early years workforce. Nearly a third of five-year-olds are not reaching a good level of development, according to their teachers, and the gap between more disadvantaged children and their peers at age five has already opened up significantly: analysis of results indicates that disadvantaged children are 4.6 months behind their peers by the end of the reception year.
Worryingly, there are also signs of serious prevailing mental health issues among parents: perinatal mental illness affects up to 20% of new and expectant mothers, according to the NHS, and more in areas with high levels of deprivation. Fathers can also be affected and this is a problem not just for parents: pre-school children of parents with poor mental health are three times more likely to have a mental health difficulty themselves than children whose parents have good mental health, and the effects can continue into later childhood and adulthood. We live at a time when mental health problems are all too common and are one of the main causes of the overall disease burden worldwide [1]. Yet Ipsos MORI found that only 10% of parents took time to look after their own mental wellbeing during pregnancy [2]. Providing as much protection as we can in the early years is our best opportunity to halt or even reverse the increasing prevalence of mental health issues, particularly among children and young people.
For some children and some families, the risk of experiencing adverse events that have negative impacts on wellbeing and development is greater than for others. The Children’s Commissioner has reported that over half a million children in England live in the most vulnerable circumstances, and we know that a far bigger group experience other forms of adversity and significant economic challenges. An estimated 1.3 million babies and pre-school children live in poverty: this represents over a third of children aged under five in the UK, and families with children under three years old face the highest risk. A number of ethnic minority groups are over- represented within this group.
The professionals who make up the early years workforce stand alongside parents as essential caregivers. Since the 1990s there has been substantial investment in early education, but there is more that could be done to strengthen the system. Building more capacity and valuing a committed workforce will help address problems with retention. Professionals also need the right support and training so that they are equipped to support the emotional and social development of under-fives, as well as their physical development.
The coronavirus pandemic has made things harder for many families with babies and young children, taking an additional toll on the mental health and wellbeing of children and parents — and the effects have been felt most by those already living in disadvantaged or difficult situations. The impacts of this particularly challenging time have started to become apparent, with an increasing number of reports of serious harm affecting the youngest children and teachers finding that the language and personal development of those starting school is often behind where it should be.
In the fourth and final chapter, ‘Opportunities for Change’, we outline the huge opportunities we have to bring about positive change in every aspect of society and for generations to come. Armed with knowledge from the science and data, we set out six practical areas of opportunity where, by working collaboratively, we can make a difference.
Summary of recommendations
Raising awareness of the extraordinary impact of the early years. Knowledge of the importance of the early years is low. We need to increase societal understanding of the transformative impact of early childhood. We also need to change the way we think about the first five years — ensuring that emotional development is given due focus and attention by all and that caregivers have sufficient understanding and knowledge to support healthy development.
Building a mentally healthier and more nurturing society Healthy development requires nurturing relationships, environments and experiences. We need to value the role of caregivers, to prioritise their mental wellbeing, starting in pregnancy, and to build their capacity and capability. Surrounding this we should create nurturing environments and experiences, including access to nature and outdoor space.
Creating communities of support. Caregivers do not exist in a vacuum; we need family-friendly communities that create non-judgemental environments, encourage help-seeking and ensure that early childhood is prioritised locally. Workplaces can also play a role, shaping a culture that supports the early years.
Strengthening the early years workforce. There are thousands of dedicated and hardworking individuals who are committed to supporting families in the early years. We need to recognise the importance of the early years workforce and to reflect this both in the quality of training and in support for their own emotional wellbeing. Where needed, we should also encourage a more holistic view of the early years that includes emotional as well as physical needs, and provide easy access to the latest scientific research to inform practice.
Putting data to work for the early years. Data on babies and infants are both patchy and unconsolidated. At the same time, there are gaps in research and in the implementation of best practice. We need to gather data routinely and consistently from birth onwards and find ways to share information between all those who provide care and support in the early years. We should undertake to build a more substantive body of knowledge, including psychological and behavioural science as well as longitudinal studies and economic evaluations. And where we have research, this should be used to inform programmes and practice.
Supporting long-term and intergenerational change. We need long-term commitment to building and sustaining an effective system which includes a national framework that will provide a common agenda to drive holistic and preventative early childhood support; deeper collaborative working; and a measurable child outcomes framework.
Chapter 1
Shaping Our Lives
A child’s physical transformation in the early years is plain to see and the ‘milestones’ that are most often recognised and measured relate to physical development: the first smile; the first steps; the first words. What we also know now from the science is the extraordinary extent to which the brain changes during pregnancy and in the first five years. This has implications for our development that go far beyond our physical abilities.
Advances in brain science over the past three decades, along with findings from psychologists and a number of long-term studies tracking large groups of children, have revealed just how profoundly early development shapes our long-term mental and physical health and influences our life outcomes. This growing body of research has also proven beyond doubt the importance of both nature and nurture. Our genes play an important role in shaping our physical attributes, as well as aspects of our personality and cognitive ability. However, genes only encode potential. How we develop across our lifespan depends on the interaction of our genes and the environmental experiences and resources that are available to us, particularly in childhood. In other words, genes only code for what could be — a blueprint for our future development [3].
For children to reach their full potential and make their blueprint a reality they need the right materials: a healthy and emotionally stable early environment enriched with opportunities and resources for growth, learning and development. While we continue to grow and learn throughout our lives, the quality and stability of our earliest relationships, as well as experiences and environments in pregnancy and early childhood, are key to shaping who we are. It is these relationships, experiences and environments that build our emotional and social capabilities and thinking skills, with implications for how our bodies work too. Writ large, this means that supporting healthy development means considering the emotional needs of babies (in utero and after birth) and infants as well as their physical needs. The way in which children are nurtured at the very start of life provides a golden opportunity for positively shaping society and future generations.
Yet while most people would acknowledge that the world in which we grow up helps shape the adults we become, the full import of the early years in laying foundations for life is not widely recognised. A comprehensive study of public attitudes across the UK published by The Royal Foundation with Ipsos MORI in 2020 found that, among UK parents, recognition was relatively low that the first five years of life are the most important for health and happiness in adulthood. Fewer than a quarter of respondents (24%) saw the first five years as the most important period in a child’s life for later health and happiness, and nearly two-thirds (64%) were not aware of the uniquely rapid period of brain development that takes place from conception to age two [4].
This chapter examines what we know from the evidence available. Being armed with knowledge should empower us all to act to support families better.
The developing brain: foundational connections
Our brain-building starts in utero and we are all born with billions of neurons — specialised brain cells designed to transmit information to other nerve cells around the body. Rapid brain growth means that by age two our brains are approximately 80% of adult weight, reaching 90% of adult size by age five [5].
Our brains are approximately
80%
of their adult weight by the age of two
However, it is the trillions of connections — our synapses — between the nerve cells, formed most rapidly in early childhood, that are key in making our brains and bodies function. Young children form more than a million synapses per second in the first few years [6]. These critical connections are shaped by our earliest relationships, environments and experiences, and it is the arrangement and strength of these initial connections that allow the development of increasingly intricate and inter-related systems in the brain [7].
Scientists at The Center on the Developing Child at Harvard University talk about the unique plasticity of the brain in the earliest years: not only is it developing quickly, but it is also dependent on, and extraordinarily receptive to, its environment [8]. The process of brain-building starts with overproduction of the cellular material required to make synapses; our bodies naturally generate more of this material than is required. Over time, connections are made (or not) based on the experiences we have (or do not have).
Repeated experiences create stronger and faster connections, while a lack of certain kinds of experience during critical periods of development can inhibit the development of connections in specific areas of the brain. For example, if the eyes do not receive visual input during the critical period for optical development, these brain areas may never function properly. Lack of activation or use can leave connections weak, and connections that are not used or strengthened die off [9]. Although this pruning process is a natural part of brain development, an absence of stable, caring relationships and enriching experiences can weaken the neural networks that underlie key thinking skills and emotional capabilities.
An absence of stable, caring relationships and enriching experiences can weaken the neural networks that underlie key thinking skills and emotional capabilities
Early, positive experiences strengthen neural connections. The critical emotional bond between a baby and its primary caregiver — often referred to as ‘attachment’ — is dependent on early, reciprocal interaction. Over time the sequential building of connections, structure upon structure, means that the nature and strength of each ‘layer’ of connections affects subsequent development.
Connections that underpin more basic processes, such as our senses and simple emotions, form first. Over time, with the right experiences, more complex circuits emerge, like those for speech and motor functions. Circuits required for reasoning and behavioural control continue to develop throughout childhood and into early adulthood. All these circuits are built on those formed in the earliest years, and so there is an opportunity to shape later outcomes by building solid foundations first. A good start makes good outcomes both more likely and easier to achieve.
New understanding about how our genes are expressed during development (i.e. how our genes are turned on and off) supports this.
Our individual DNA blueprint does not change, but in recent years scientists have been learning that gene expression can be altered by experience. This field of epigenetic research is at an early stage; however, it may provide a further key to unlocking how early adversity can increase the risk of poor outcomes [10].
Knowing that development is not a pre-determined process empowers us all to play our part in creating better emotional, social and physical environments for babies and young children. We need to harness this unique opportunity to help them to thrive in the first five years.

Early development affects life outcomes
Longitudinal research tracking large numbers of children over time provides proof that brain development in the early years, supported by stable, caring relationships, positive experiences and enriching environments, has a big impact on life outcomes and helps to shape our society.
One of the most compelling longitudinal studies looking at how the early years affect life outcomes has been the Dunedin Study in New Zealand. Tracking 1,000 people from birth in 1972-73, this study has examined the nature and prevalence of development and health problems over almost five decades [11]. It is still ongoing, but its findings so far demonstrate a compelling association between early childhood and development and outcomes in earlier and later adulthood. They show, for example, that displaying self-control — the ability to manage emotions — is more important than socioeconomic status or IQ in predicting adults’ physical health, parenting of the next generation, life satisfaction, wealth or factors such as addiction and crime. Children who at age three had developed strong self- control were as adults less at risk of health problems, and were more likely to be financially secure and less likely to have been convicted of a criminal offence [12].
We know that exposure to adverse experiences in the early years has the potential to create vulnerability to mental and physical health problems in childhood. For example, pre-school children of parents with poor mental health are three times more likely to have a mental health difficulty than children whose parents have good mental health [13]. We also know that these vulnerabilities can last into later life [14,15]. When the participants in the Dunedin Study were aged 32 they were assessed for the presence of biological indicators for the risk of major depression, high inflammation levels (which can lead to chronic illness) and heart disease. What the research showed was a clear and elevated risk for mental and physical ill health among those who as children had been exposed to adverse experiences such as socioeconomic disadvantage, maltreatment or social isolation.
A variety of scientific disciplines are increasing our understanding of what happens when the young brain and body are exposed to negative or adverse experiences that are not counteracted by sufficient support. In the 1980s and 1990s, electrophysiology (monitoring the electrical activity of neurons) was first used to examine brain activity in individuals who had suffered maltreatment, including abuse and neglect. Since then, magnetic resonance imaging (MRI) has been transformative in documenting how early adversity can affect brain structure, particularly during the prenatal period and in the first few years after birth. In the past decade, research using functional MRI has demonstrated that adverse experiences can alter how a child’s brain works — specifically, how the brain processes negative (‘threatening’) and positive (‘rewarding’) aspects of the environment and how emotions are regulated [16]. These altered patterns of brain function may be helpful for a child in the short term in an adverse home environment, but they have the potential to create latent or underlying vulnerabilities that affect mental health, social development and learning over time.
Maternal depression, particularly in pregnancy and during the first year or two of a child’s life, interferes with a mother’s ability to interact with her child and to provide protection from other sources of stress, and this, in turn, has been shown to affect a child’s stress response. There is increasing evidence that these effects are one mechanism linking maternal depression to the child’s own risk of developing depression and other emotional disorders. Studies of infants with mothers suffering from depression show patterns of brain activity similar to those found in adults with depression [17].
Research has also shown that children who have experienced physical abuse or domestic violence exhibit patterns of brain reactivity when they process threat cues reflecting hypervigilance, similar to those observed in soldiers exposed to combat [18]. By adulthood, early brain adaptations of this kind may continue to influence how an individual negotiates their social world. One instance of this is the condition known as complex post-traumatic stress disorder (C-PTSD), which has recently been recognised internationally [19]. This is a common, long-lasting and disabling condition similar to PTSD, and is strongly associated with childhood adversity.
Research has also shown that children who experience maltreatment are more likely as adults to experience more interpersonal stressor events, have smaller social networks and experience greater loneliness and lower levels of social support [20,21]. This pattern of loss of social networks is a compelling demonstration of the long reach of childhood adversity — how our experiences early in life have profound impacts on our lives as adults, and ultimately as parents [22].
The wide-ranging and long-term outcomes of early development are also borne out by a working paper from The Center on the Developing Child at Harvard University, Connecting the Brain to the Rest of the Body [23]. This explains that while adverse experiences are processed by the brain, the effects are not limited to that organ but are also physiological, cascading through the body’s interconnected systems. Responses are triggered in the nervous system which automatically lead to increases in heart rate and breathing. Hormones are regulated and rebalanced to respond to threat. The immune system prepares itself to protect and repair, and metabolic systems react by releasing more energy to fuel the body. As the paper explains, the brain and all other organs and systems in the body are like a team of highly skilled athletes, each with a specialised capability that complements the others and all of which are dedicated to a common goal. Peak performance of the team is more easily achieved if all its members can optimise their individual effort and can learn to work together.
Inflammation is a common and natural consequence of the immune system’s response to all forms of stress. However, prolonged stress weakens the immune system, leading to prolonged inflammation and making the body more prone to chronic conditions that manifest later in life, including heart disease, depression, arthritis, gastrointestinal disorders, autoimmune disorders, multiple types of cancer and dementia.
In the cardiometabolic system, for example, excessive amounts of stress hormones like cortisol combined with chronic inflammation can result in insulin resistance. Inflammation also interferes with blood flow to the heart in adults by causing the build-up of plaque on the walls of the arteries. The implications of this research are far-reaching. It seems that early experience of chronic stress can contribute to an increased risk of long-term mental and physical health problems including depression, obesity, diabetes and cardiovascular disease, [24, 25, 26] with the associated human and societal costs.
The important message from the science is that there is a golden opportunity to act in the first five years, when the brain has greater plasticity. However, experiencing adversity in early childhood is not determinative and the early years are not the only opportunity to act — support can, and should, be provided throughout life.

Building a healthy brain
The more we learn about early emotional, social and cognitive brain development, the clearer the imperative becomes to all of us to harness this key moment. So the question is, what can we do about it? At the most basic level, what shapes our brain and development most significantly in our first five years is the relative balance of two things: the positive and protective factors that nurture us and buffer us and our exposure to adverse experiences.
Positive and protective factors are the relationships, environments and experiences that support healthy brain development. These factors are key in helping infants to develop and learn how to regulate their emotions, feelings and behaviour, and build their sense of agency and resilience and their confidence to independently navigate their physical and social worlds.
Challenging and, sometimes, negative experiences will occur in the course of our lives, and during early childhood our brains and bodies develop to deal with them. Learning to cope with experiences that cause moderate stress (for example, meeting a stranger or starting at nursery), with the support of a caregiver, contributes positively to development. A secure relationship with an adult can also buffer a child against the effects of longer-lasting and more severe stress (for example, the loss of a loved one) and therefore protects the developing brain from the potentially harmful impact of trauma [27]. In this way the effect of negative experiences can be made tolerable.
When children grow up without healthy, nurturing care (for example, due to parental mental illness or addiction), with prolonged and uncontrollable adversity (for instance, as a result of physical and emotional neglect, maltreatment, poor nutrition, socioeconomic hardship, discrimination, pollution or parental mental illness and addiction) or without supportive relationships, over-activation of the stress response over long periods of time can become harmful, with potential long-term effects; this has been described by the Harvard scientists as ‘toxic stress’.
The role of parents
The importance of the relationship between a child and their primary caregiver has long been understood, [28] and research continues to show the positive impact of nurture. For children to be nurtured, they need nurtured adults around them.
A stable and stimulating home environment, with a wealth of parent–child interactions, is associated with early cognitive and language development, performance in IQ testing and later achievement in school. Sensitive and responsive parent–child relationships — which lead to secure attachments — have been shown to be associated with enhanced social competence and stronger cognitive skills in babies and young children [29]. Healthy development is supported through the simplest interactions with children, engaging with them and responding to them. These interactions fire neural signals in the child’s brain and, over time, contribute to strong and fast connections.
Children need to learn how to self-regulate and, until a child’s brain has capacity to regulate emotion independently, the caregiver is an essential source of external regulation, helping the child to manage their emotions in the face of external sources of stress. Children who have this kind of experience of ‘co-regulation’ with their primary caregiver are better placed eventually to acquire the ability for independent emotional self-regulation, which is essential to enable them to focus their attention and to learn.
Self-regulation is just one of many inter-related skills that, with nurturing care, are built over time and through practice. Developing what are called ‘executive function’ skills is crucial for both cognitive and social capacities. These give children (and later when they are adults) the ability to self-control and manage impulses, to remember and manipulate information over short periods of time, and to adjust to changing demands, priorities or perspectives. With the right support, the development of executive functioning accelerates between ages three and five, and continues to develop into early adulthood [30]. Young children depend on their emerging executive function skills as they sustain play with their peers, take part in organised activities and learn to read and write.
Carers’ awareness of the baby and infant as a person with their own thoughts and feelings enables them to provide sensitive care and to create a secure and trusting bond with the child. The nurturing parent looks beyond the child’s actions and tries to see what they may be experiencing. Psychologists have talked about this as ‘mind-mindedness’ or ‘mentalising’. This form of sensitivity appears to have beneficial effects not just in terms of the parent–child relationship but also for the child’s cognitive and emotional development [31].
The wider support network
Primary caregivers play the most critical role, but they do not exist in a vacuum and their capacity and ability are inextricably linked with their own experiences when they were growing up and with the support they receive, as adults, from the communities around them. Parents need support from both inside and outside the family, and this is even more important for those who themselves did not experience the best start in life.
Professionals, (including midwives, health visitors, GPs and childcare workers) and family and friends, will help define the relationships, environments and experiences that children are exposed to. So it is vital that they have access to the right knowledge and skills to nurture children, and they need support for their own emotional wellbeing too.
The surroundings in which a child is brought up, the available nutrition and healthcare, the quality of relationships between adults and the relationships that are formed between caregivers and infants are all-important. Relationships, environments and experiences that babies and young children encounter both in and beyond the home can also make a positive difference to how they develop in the long term. These include safe spaces that support learning and social interaction, green outdoor spaces that allow exercise and physical activity and environments free of pollutants.
Longitudinal studies have also looked at the role of childcare and early education. An influential early piece of research in this area was the Perry Preschool Study in the US, which began in the 1960s. This project illustrated how high-quality pre-school education can make a dramatic difference to children’s developmental chances by tracking the outcomes of 123 participants from low-income African-American families, half of whom were provided with high- quality pre-school education. It found that positive experiences in early childhood supported both social and intellectual development, with positive effects on school performance that were still in evidence, years later, into adulthood. The participants who received the pre-school education had fewer teenage pregnancies and were
more likely to have graduated from high school, to hold a job and have higher earnings, to own their home and car and to have committed fewer crimes [32].
More recently in the UK, the Effective Pre-School, Primary and Secondary Education (EPPSE) study followed nearly 2,600 children from early childhood in the late 1990s to the age of 16. Positive effects on child outcomes were seen throughout primary and secondary school, including better intellectual development. The study also showed that the quality of the pre-school setting was an important factor in determining positive outcomes, particularly for children from disadvantaged backgrounds [33].
Parents need support from both inside and outside the family, and this is even more important for those who themselves did not experience the best start in life
Building resilience
Our understanding of the developmental process will continue to evolve, but it is clear from the science and the wider research presented here that the early years present a golden opportunity to support both physical and emotional development, with benefits for mental health and wellbeing through the whole of life and across generations. Children who are able to benefit from positive and nurturing relationships, experiences and environments and who are protected from external sources of adversity enjoy the prospect of better outcomes in life. They have solid foundations to support their mental and physical health and to promote good educational attainment and long-term material stability. They are also better equipped to develop the social and emotional capabilities that are needed for healthy relationships, and to build resilience to weather future adversity and meet the challenges of parenting themselves.
This all underlines just how much parenting in the early years really matters. As our Ipsos MORI research showed, most UK parents (73%) find it a stressful time when their child is under the age of five [34]. Primary caregivers do not exist in a vacuum and they need support with their knowledge, skills and emotional wellbeing. The nature of that support varies enormously between families and over time. Those in poverty, or parents struggling with their mental health or with addiction, face extra challenges that make it more difficult to provide the kind of nurturing care that is essential to a good start in life.
73%
of UK parents find it stressful when their child is under the age of five
We all have a part to play our part in providing the right experiences and environments for babies and young children. It is imperative to consider how we support and develop the professional workforce and build family-friendly policies and communities that support all caregivers. We also need, so far as possible, to remove obstacles and reduce the effects of adversity, enabling every individual to thrive, from pregnancy to age five.
The following chapters explore further where we are now and the opportunities that exist to meet this challenge.
Chapter 2
The economics of the early years
As the science and research set out in Chapter 1 make clear, the way in which children are nurtured at the very start of life provides a golden opportunity for positively shaping society and future generations. Conversely, when parents lack support and their children miss the opportunity to develop healthily during pregnancy and up to the age of five, the personal and human costs can be great, and the effects on the individual reverberate across society. If not addressed, these effects can influence the way we relate to one another and function as a community and, potentially, the whole country’s long-term economic success. Economists started looking at the financial opportunity of investment in early childhood in the 1960s, and there is a growing body of research in this area. This chapter looks at the economic case for acting in the early years.
An opportunity to save billions of pounds
Long-term studies have looked at how the early years affect life outcomes. For example, the Dunedin Study in New Zealand, mentioned earlier, has demonstrated a clear association between early childhood and development and outcomes in later childhood, adolescence and adulthood [35]. The effects of early adversity might be felt in terms of poor mental health and wellbeing, compromised physical health and a host of social challenges, from a lack of educational attainment to joblessness and from addiction to homelessness.
In the UK, and around the world, the prevalence of mental health issues has been increasing in recent years. Research conducted by the National Centre for Social Research with the University of Leicester found that one in six (17%) of people over the age of 16 had a common mental health problem in 2016 [36]. In 2017, one in eight (12.8%) of five- to 19-year-olds in England was found to have at least one mental health disorder [37]. A focus on the early years offers an opportunity to address the issues that make children vulnerable to developing later mental health problems that reduce their chances of enjoying a fulfilling life. Given in particular the challenges that await the new generation of (post-pandemic) children, we need to provide children and young people with as much protection as we are able to if we are to halt or even reverse the increasing prevalence of mental health problems.
Building an informed picture of the costs of poor mental health and other long-term outcomes associated with the early years helps us to understand more about the opportunity and the extent of the savings that might be realised through a greater focus on early childhood development.
The Royal Foundation of The Duke and Duchess of Cambridge commissioned the London School of Economics (LSE) to look at the most recent data on public expenditure. The LSE’s study has produced an estimate for 2018/19 of lost opportunities in the early years i.e. expenditure that might reasonably be avoided or replaced if preventative action were taken in early childhood. The estimate includes long-term expenditure associated with adverse childhood experiences (ACEs), taking into account population attributable fractions (PAFs), i.e. the fraction of expenditure related to the problem in question that might be causally linked to ACEs [38]. It calculated that the costs associated with lost opportunity in 2018/19, in England alone, were in the region of £16.13 billion [39].
£16.13 billion
The cost of lost opportunity in England
To put this spend into perspective, £16.13 billion a year represents:
Nearly five times the total annual spend on early education
and childcare entitlements [40]Around 44 times the investment in specialist perinatal mental
health services between 2015/16 and 2021. [41]
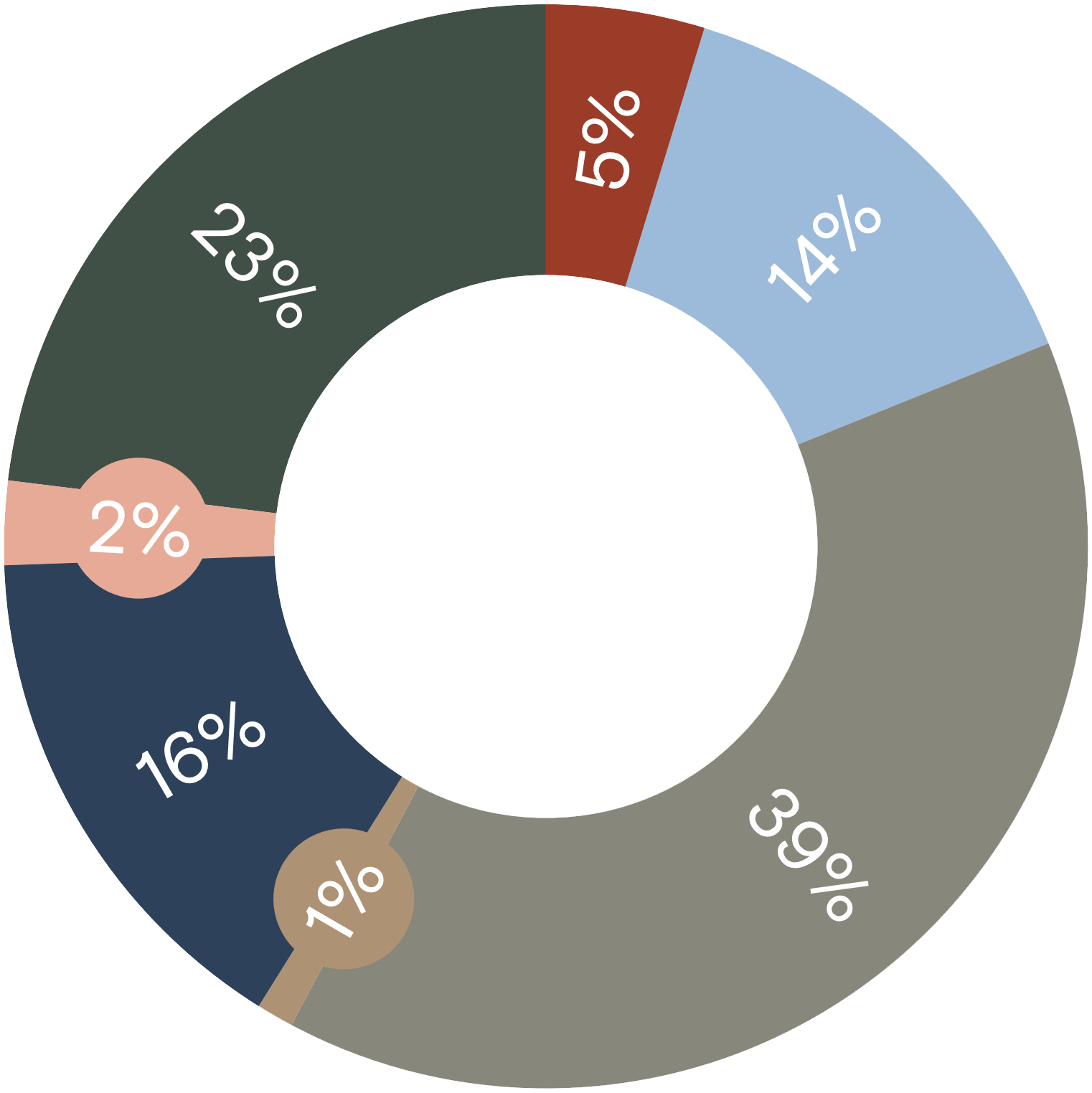
The categories of cost within this figure include child injuries and mental health problems; children’s social care; crime and antisocial behaviour; school absence and exclusions; and youth economic activity. The analysis also includes the costs of long-term mental and physical health and some long-term social consequences (such as homelessness), taking into account (for some categories of cost) the proportion of expenditure likely to be attributable to ACEs.
| Category of expenditure | Cost | |
|---|---|---|
| School absence and exclusions | £770,000,000 | |
| Youth economic inactivity | £2,290,000,000 | |
| Children’s social care | £6,270,000,000 | |
| Child injuries and mental health problems | £200,000,000 | |
| Crime and antisocial behaviour | £2,514,000,000 | |
| Long-term health consequences of ACEs | £411,000,000 | |
| Mental health and social consequences of ACEs | £3,670,000,000 | |
| Grand total | £16,125,000,000 |
This is the cost to society of the remedial steps we take to address current issues — from crime and antisocial behaviour to long-term mental and physical health issues — that might have been avoided through action in early childhood.
The LSE analysis does not suggest that it is possible to avoid the entire £16.13 billion of costs, and indeed some expenditure will always be necessary. However, avoiding the need to spend even a fraction of this £16.13 billion justifies a greater focus on early action and prevention. Of course, focusing our efforts earlier and saving some of the substantial costs of remedial action requires investment upfront and a shift back to early support and preventative services. In this context there is increased momentum for addressing this balance of priorities. Investing in the early years is a mission that can unite communities, leaders, businesses and families.
Uncounted costs
It is important to understand that the figure of £16.13 billion is an estimate and that it reflects only expenditure that can be relatively easily extracted from routine data. This means that there are costs that are not included in the total, most notably the costs of some of the long-term social consequences of early adversity, including those associated with persistent criminality. The figure may also under-represent expenditure on mental health as it is difficult to identify all those costs that relate to the early years [42]. In addition the LSE analysis, focusing as it does on what is currently spent in England on lost opportunity, does not factor in the cost of unmet need.
Looking at the economic case more broadly, it is also notable that the studies tracking cohorts of children over time have shown that childhood maltreatment has significant impacts on adult economic productivity, [43] and other indirect costs include lower earning potential, costs associated with persistent criminality and the knock-on costs of health and social problems to friends, family and the next generation. In total, these costs are likely to dwarf the £16.13 billion.
Where to invest?
In addition to knowing that there are substantial costs that we might be able to save by acting in the early years, there is a growing body of evidence about the type of support that is effective, in terms of both improving outcomes and delivering a measurable return on investment.
The weight of evidence suggests that the case for investment is strong both at the level of individual programmes and at a wider systemic level, though there is much more evidence available in relation to the former. System-wide interventions can be hard to evaluate but evidence has shown, for example, that in England the presence of Sure Start children’s centres, offering multi-agency support to families, helped save healthcare costs when those costs were looked at in later childhood [44]. At a programmatic level, a number of areas are beginning to produce a substantial body of evidence of positive benefit. These include early education and childcare, perinatal mental health support and parenting support programmes [45].
Mental health support for mothers
Economic evaluations also suggest that training professionals in universal health services, such as training health visitors on systematically assessing women’s mental health problems and providing or arranging for psychologically informed support techniques, is also likely to be cost-effective [46, 47]. In addition to improving maternal outcomes, findings from the studies suggest that treatment might potentially achieve positive impacts on the infant, such as improved sleep or temperament as well as child development or behaviour [48, 49]. Treatments that have been shown to be cost-effective include cognitive behavioural therapy (CBT), interpersonal therapy (IPT) and guided self-help. Working with infants and mothers together can help with infant attachment where a mother is suffering from postnatal depression, and is potentially also cost-effective [50].
Early education and childcare
The economic benefits of high-quality, universal early education and childcare, particularly for children who lack a rich home learning environment and who live with deprivation and other disadvantages, have been widely acknowledged.
Much of the evidence on cost-effectiveness or cost-benefit from a life course perspective comes from the US, and Professor James Heckman’s research on pre-school education programmes is often cited as making the case for investment in early childhood development [51]. In 2016 new research [52] was published by his team, based on an analysis of the long-term outcomes of children who had attended intensive pre-school programmes in North Carolina in the 1970s. The programmes offered comprehensive developmental resources to disadvantaged African-American children from birth to age five, including nutrition, access to healthcare and early learning. The research looked at a wide variety of life outcomes (measured well into adulthood) such as health, the quality of life, involvement in crime, income, schooling, academic attainment and increases in mothers’ income due to subsidised childcare. The research concluded that high-quality programmes for disadvantaged children, from birth to the age of five, can deliver a potential 13% return on investment annually, through childhood and adulthood. Many more children attend pre-school now in the UK than they did in the US in the 1970s and so the return on investment for the current generation of under-fives may be less than 13% per year, but it may still be close to the kind of significant return of 7–10% identified in other research where the right level of quality can be achieved [53]. Recent research in Europe and the UK has further enhanced our understanding in this area, highlighting that short-term impacts from early education and childhood can sometimes be ‘washed out’ in later childhood only to re-emerge later in adolescence and adulthood, and that the quality of provision accessed by a child is absolutely critical for longer-term benefits [54].
Equipped with this kind of information, we can evaluate the opportunities created by taking action in the early years and make informed and balanced decisions about the type of support that we should prioritise.
High-quality programmes for disadvantaged children, from birth to the age of five, can deliver a potential 13% return on investment annually, through childhood and adulthood
Chapter 3
Where we are now
Chapters 1 and 2 have shown us how important the early years are for shaping children’s early development and influencing their life outcomes. They show also the potential long-term benefits to individuals and the economic opportunity for the whole of society created by effective support for children and families in the early years.
In this chapter we consider the state of play for babies, young children and their parents and caregivers in the UK today and the current support they receive.
Parenting is an enriching experience for most, but many parents — both mothers and fathers — suffer from loneliness, stress and poor mental health during pregnancy and beyond. A significant number of young children are showing signs of mental ill health and many children are not reaching a ‘good level of development’ by the age of five. Many families, including those who are in work, are struggling financially and with other forms of adversity, and for many the COVID-19 pandemic has made problems worse. Yet there are signs of an increasing focus on the early years from across the political spectrum, which can be built upon.
It will take action from all of us to realise the benefits of healthy early childhood development. Across the world, nations are recognising the need to do more. Reflecting this, in 2018 the World Health Organization (WHO) published the Nurturing Care Framework for Early Childhood Development [55]. There are also some positive indications that, despite the many challenges posed by the COVID-19 pandemic, during this period families have started to feel more supported by their local communities. However, the evidence marshalled here suggests that we all have more work to do.
A 2015 review of studies from Europe (including the UK) and the US estimated that almost one in five (17%) of children under six experience mental health problems
Young children’s developmental outcomes and the attainment gap
At the end of the first year of school in England, all children are assessed against the Early Years Foundation Stage (EYFS) profile, which looks at early learning goals (including communication and language; and social and emotional development) and characteristics of effective learning (playing and exploring; active learning; creating and thinking critically). The latest published figures for 2019 [56] show that on average in England almost a third (28.2%) of children do not reach a ‘good level of development’ by the age of five [57].
28%
of children in England do not reach a ‘good level of development’ by the age of five
EYFS results also indicate that children from low-income families are less likely to develop positively across the range of measures by the end of reception compared with their peers. Analysis of EYFS results finds that disadvantaged children are on average 4.6 months behind by the end of the reception year [58]. Further, the Office of the Children’s Commissioner reports that up to 40% of children living in disadvantaged households are now not reaching a ‘good level of development’ by the age of five, and one in seven (14.3%) — equivalent to about 82,500 children a year — fails to meet more than half their developmental indicators in reception year [59]. These are children who are starting school significantly behind in their physical, emotional and social development.
As discussed in more detail below, there are signs that the pandemic has further widened the gaps for a generation of children who have missed out on significant time in nursery. In a 2020 survey, Key Stage 1 teachers reported that, on average, 46% of children aged four or five had arrived for their first year in reception not ‘ready for school’ (in contrast with 35% in 2019) [60]. While there is no single definition of ‘school ready’, the types of issue that teachers identified included children who did not know how to listen or to respond to instruction; who struggled to play or to share with other children; who could not hold a pencil; and who were not able to eat independently and/or who were not toilet-trained.
We know that this will have long-term consequences: the evidence shows that gaps at school entry lead on to a sizable share of gaps in later achievement. One recent study found that more than half of the gaps in achievement at age 11 are due to inequality that was already present at age five [61].
46%
of children aged four or five arrived for their first year in reception not ‘ready for school’
Mental health outcomes for under-fives
Measuring early development outcomes across the population is hard, but there are some early indicators internationally that some young children are experiencing mental health issues early in life. A 2015 review of studies from Europe (including the UK) and the US estimated that almost one in five (17%) of children under six experience mental health problems, with more than half of these children being severely affected [62]. A 2017 study identified that one in 18 (5.5%) of two- to four-year-olds in England had signs of diagnosable mental ill health [63].
Parental mental health and wellbeing
Parental wellbeing is the biggest single factor for a child’s wellbeing. If a parent is struggling, this will have harmful impacts on their child. Yet since the 1970s the majority of empirical studies conducted in industrialised societies have found a lower level of emotional wellbeing amongst parents — both mothers and fathers — compared with non-parents.
For a significant number of parents, wellbeing is more seriously compromised. Many parents in the UK suffer with mental ill health problems and loneliness, and have few people to whom they can turn for help or who they trust to help. Perinatal mental illness affects up to 20% of new and expectant mothers, according to the NHS [64], rising to up to 25% of women in diverse urban areas [65]. This is not just an issue for mothers: around 10% of all new fathers also have a common mental health problem [66].
Parental wellbeing is the biggest single factor for a child’s wellbeing. If a parent is struggling, this will have harmful impacts on their child
We know that when parents who suffer with poor mental health are not helped, or not helped early enough, their ability to engage with their children is compromised. A caregiver who is chronically depressed might be withdrawn or disengaged and unable to interact with their baby or young child. Untreated perinatal mental illnesses are also the leading cause of death for women during pregnancy and the year after birth. Both maternal mental health problems and their effects on relationships with babies are treatable, but we know that we can continue to improve the care provided for mothers.
Spotting the early signs that a mother is struggling allows us to provide the right support early on and the possibility of preventing mild symptoms from becoming severe. The early years workforce needs to be equipped to recognise when a mother needs help and understand how mental ill health affects their ability to create a secure attachment between mother and child. Family and friends need to be aware of the signs to look out for (and this is as true for fathers as it is for mothers) and can encourage outreach to peer support groups or health professionals. With this in mind, we also need to boost the emphasis on trauma-informed care in national perinatal mental health strategies, with more of a focus on mothers who have mild to moderate mental health issues.
20%
of new and expectant mothers are affected by perinatal mental illness
The most vulnerable
A significant minority of children experience severe adversity. For some, this may relate to being born with a learning or physical disability: there are estimated to be 118,000 children under five in the UK with a learning disability, and they face increased risk of poor outcomes on a host of indicators [67, 68]. For others, it may relate to the situation of their parents. In the UK today many are affected by the ‘toxic trio’ of substance abuse, domestic abuse and mental illness. The Office of the Children’s Commissioner currently calculates that 549,700 children in England alone under the age of five live in these most vulnerable of family circumstances [69]. Those children most at risk of living with this trio of factors are those whose parents themselves experienced adversity in their own early childhood.
Economic challenge and poverty
There is a far broader constituency of families experiencing significant economic challenges. Analysis by the Joseph Rowntree Foundation has shown that relative poverty has risen most rapidly over the past decade for households where there is a child under five. An estimated 1.3 million babies and children under the age of five in the UK now live in poverty — this represents a third (34%) of all families with a child in this age group. Families with a child aged under three face the highest risk [70].
1.3m
babies and children under the age of five in the UK now live in poverty
Over the past 20 years the most noticeable change has been the shift in families’ circumstances. Now the majority (70%) of people living in poverty are from working families [71]. The realities facing many young families are that wages are stagnant, jobs are insecure and housing and childcare costs are very high relative to income [72]. Families are increasingly likely to need two incomes, just to get by. But even with both parents in work, it is often not enough.
Economic hardship affects every aspect of family life. It is associated with greatly increased risks of poor housing, overcrowding, food and energy insecurity, poor nutrition and lack of play opportunities. Parents in this situation are naturally less likely to have the capacity to provide the positive home environment and experiences that their babies and young children need. And these factors in turn are linked to poorer childhood development on a host of measures, as well as later mental and physical health inequalities [73, 74].
Ethnic disparities
We know that addressing disparities across communities presents one of the most significant opportunities for improvement. The Millennium Cohort Study has shown that there are large ethnic gaps in early child development. To a great extent, these gaps are a reflection of broader inequalities. In England children in Asian (37%) and Black (37%) households are twice as likely to live in persistent low-income conditions as children in White households (18%).
They are also significantly more likely to have had lower birth weights than White children, and disparities are reported in rates of depression among mothers during the child’s first year, reflecting wider mental health disparities [75]. More work is needed to understand the drivers of all of these disparities.
In England children in Asian and Black households are twice as likely to live in persistent low-income conditions as children in White households
Parental leave
Parental leave and flexible working can make a big difference to the quality of care that parents are able to provide — particularly to those on low incomes. Parental leave rights in the UK and across Europe have been strengthened over the past few decades. However, making a comparison across full-rate equivalent weeks of paid maternity leave, the Organisation for Economic Co-operation and Development (OECD) has found that the offer to families in the UK is less than those in Germany, France, Australia, Spain, the Netherlands and Italy, although considerably ahead of the US [76]. This is an area where employers as well as policy makers could make a significant difference.
Parental loneliness and stigma
Parenting in the UK can feel lonely. The Jo Cox Commission on Loneliness reports that more than half (52%) of UK parents have suffered from loneliness — with a fifth (21%) having felt lonely in the previous week [77]. One in five parents (18%) reports that they have at most two people they can turn to locally for support if needed, and many say that the number of people in their network has decreased since they have had children [78]. For a considerable number of parents, the perception is that social and community support is simply not enough.
52%
of UK parents have suffered from loneliness
Many parents do not feel confident enough to access or accept help, for fear of judgement or stigma. The Royal Foundation’s own research highlights that some 70% of parents feel judged by others, with over half feeling that this judgement has a negative effect on their mental health [79]. This adds to a wealth of similar findings on barriers to parents asking for help. Research has found that parents sometimes feel uncomfortable about using services aimed at low-income families [80]. There is also broad evidence that fear of perceived stigma from health professionals such as health visitors can be a barrier to parents asking for help when they need it [81, 82]. Given the passion and expertise of health visitors in the UK, however, removing these barriers presents a significant opportunity to make better use of existing resources for the benefit of parents and professionals alike.
Many parents who are users of mental health services report experiencing stigma and discrimination and consequent difficulties relating to custody and parental responsibility [83]. A survey by the National Childbirth Trust (NCT) found that most mothers felt unable to talk to professionals about mental health problems because they were afraid of their reaction [84]. Self-stigma (where social prejudices about mental health difficulties are internalised to become self-critical thoughts) can be a significant barrier to seeking help and getting the right kind of advice, not only for problems related to mental health but for general parenting support as well [85].
Taken as a whole, the evidence tells us that society needs to go further than simply making support available. Ensuring that the door is truly open for parents to seek help, that they trust and are confident in services and feel welcomed and encouraged to reach out are all equally important.
For a considerable number of parents, the perception is that social and community support is simply not enough
A strong early years workforce
Through pregnancy to the age of five, children and families are supported by a passionately committed and professional workforce, including midwives, GPs, health visitors, childcare workers and educators.
In some parts of the professional workforce there is an increasing focus on developing a holistic understanding of early childhood development, looking beyond physical development to the emotional development of the child and the mental wellbeing of parents. For example, the Royal College of Midwives has developed a Maternal Emotional Wellbeing and Infant Development Guide. Releasing an updated version in 2021, the RCM commented: ‘The mental health and wellbeing of pregnant and new mothers is now acknowledged to be as important as their physical health, which has traditionally been the focus [86].’ It is vital that all practice is informed by the latest science and research.
Indeed, there is an opportunity for the UK to build a world-leading early years sector. Since the late 1990s there has been significant investment in early education. Currently, in England all three- and four-year-olds are entitled to up to 15 hours a week of free childcare and early education, for up to 38 weeks a year, with an extra 15 hours offered free to eligible working parents.
There is also a targeted offer of 15 hours of free childcare for around 40% of two-year-olds. Some support is also provided to parents directly through the benefits and tax system.
However, analysis suggests a ‘crisis in recruitment and retention in the early years sector with qualified and experienced staff leaving the sector due to poor salaries and conditions’ [87]. Research shows that staff turnover is running at 15%, and the pandemic has put further financial strain on the sector and risks worsening the situation [88].
Moreover, families’ access to health services can be affected by a lack of capacity in the system. Although health visitors are seen as an essential part of the Healthy Child Programme, between 2015 and 2017 their numbers fell by 20% [89] and they have continued to decline, leaving many of those who are still practising with extremely high caseloads. The optimum maximum caseload for effective practice is 250 children per health visitor, and fewer in areas of high vulnerability. However, the average caseload is currently closer to 500 children, and 12% of health visitors have responsibility for over 700 children [90].
The data gap
We currently have no way of reliably tracking the development of children until they reach school. In theory, data on development are available from the Ages and Stages Questionnaire (ASQ) check that takes place at two-and-a-half years of age and the EYFS pre-school check. However, problems with these datasets include low rates of completion of the ASQ and a lack of focus on social and emotional development in the pre-school EYFS check. This means that we are missing opportunities to identify issues and provide the right protective support early on, in the critical first five years.
An increasing amount is known about the kinds of early and preventative support that are effective and can deliver better outcomes. The existing network of What Works Centres is a good mechanism for consolidating the evidence base and making it accessible to all who work in the early years sector. However, we often struggle to understand why programmes that have worked well in one place and with some children and parents do not work so well elsewhere. We often lack the information and time that we need to evaluate the long-term impact and economic effectiveness of the support that is provided.
The pandemic
The coronavirus pandemic has made things harder for everyone. Depression rates in the UK have doubled, and in a UK-wide survey six in ten new parents shared significant concerns about their mental health because of the additional stress the pandemic has caused [91,92]. Additionally, in a national survey of professionals who work with babies and toddlers, 98% of respondents reported that those they support had been affected by parental anxiety or stress and by depression affecting bonding and responsive care during and after the first national lockdown [93].
And yet pregnant women and new parents have had limited access to services at a critical time in their lives. During the pandemic, many health visitors were redeployed to the frontline, children’s centres closed and professionals such as social workers, perinatal mental health workers and providers of early help were often not able to provide face-to-face support, meaning that some of the youngest children became in effect ‘invisible’ to services [94]. Research has shown that children who continued to access early education and childcare throughout the repeated lockdowns continued to develop positively in their language and key thinking skills [95] — but this was not the case for the majority.
The stress of lockdown has been worse for some families than for others. Some, for example, have reported positive effects such as children benefiting from more time spent with their fathers, and 40% of parents reported that their local community had become more supportive [96]. Yet at the same time, two in five families (38%) with babies and pre-school children have seen a reduction in their earnings since the COVID-19 crisis began, [97] and many have been forced to use food banks for the first time. In the year between 1 April 2020 and 31 March 2021, food banks in the Trussell Trust’s UK-wide network distributed 2.5 million emergency food parcels to people in crisis, a 33% increase on the previous year. Some professional groups have also highlighted the added risk of perinatal anxiety and mental health issues amongst some ethnic minority parents and parents-to-be during the pandemic, relating to the disproportionate effects of COVID-19 on different groups and a greater likelihood of it leading to hospitalisation during pregnancy [98]. Young children with disabilities and additional support needs will also have been disproportionately affected [99].
38%
of families with babies and preschool children have seen a reduction in their earnings since the COVID-19 crisis began
Some tragic consequences for the wellbeing of the youngest children during this period have already started to emerge. In 2020 there was a 30% increase in the number of notifications of serious incidents involving babies in their first year (defined as the death of, or serious harm to, a child where abuse or neglect is known or suspected) [100]. Beyond this, it is too early to say what the long-term impacts of the pandemic will be on the youngest children. Yet there is reason to believe that many in this generation will experience further negative effects over time. Teachers have already reported noticing differences, with children who started reception in September 2020 needing more help with personal, social and emotional development and with communicating than children in previous years [101].
This chapter has touched on the range of issues that undermine early childhood development today. In a world of modern pressures, we cannot expect families always to thrive or to provide nurturing relationships, experiences and environments without wider support. As the saying goes, it takes a village to raise a child.
Chapter 4
Opportunities for change
The previous chapters demonstrate the unique potential of the early years and the huge opportunity we have to make positive change in every aspect of society and for current and future generations. We all have a role to play in realising this ambition. The post-pandemic context provides both an opportunity and an urgent imperative to act. And recent focus from across the political spectrum provides reasons to be optimistic. Indeed, improvements in the system for early years support are mentioned in the government’s Early Years Healthy Development Review Report, spearheaded by Andrea Leadsom, and published in March 2021 [102]. This was followed by a commitment to prioritise support for the early years in the May 2021 Queen’s Speech.
So what might a future that embraces the extraordinary potential of the early years look like? We believe that there can be a world where a child’s emotional development is on a par with their physical development and where our mental health is seen as being as important as our physical health: a world where there is greater empathy and compassion; where we understand ourselves better; where our relationships are stronger and people do not struggle with addiction, joblessness, homelessness and violence. This world would benefit our whole society and economy, as well as each individual.
The science tells us that the roots of such a society are to be found in early childhood. Getting the early years right is of course not a panacea for all problems — but it is one of the best chances we have to significantly influence future health and wellbeing. It is a golden opportunity to set children on a stable track to adulthood and to lay solid foundations for the next generation of parents. As we consider what we want our future to look like, we have an opportunity to think afresh and to help build the society that we want to live in.
With this wind in our sails and armed with the knowledge from the science, we can make a difference. The Royal Foundation Centre for Early Childhood will focus on researching, campaigning and collaborating to raise awareness of and action on the transformative impact of early childhood. This chapter sets out six practical areas of opportunity where wider society has a role to play in harnessing this opportunity.
1. Raising awareness of the extraordinary impact of the early years
Currently, awareness of the science presented in this paper is low. Educators, experts, professionals and organisations who understand the early childhood years all have a role to:
Improve understanding of why the early years matter, including helping to translate the science, and explaining what people can do that makes a difference and what works to deliver better outcomes.
Change the way we think about early childhood to highlight the importance of the emotional development of infants and the wellbeing of caregivers. Attention should be given to good emotional development as well as to good physical development. We need a more holistic approach that goes beyond a focus on childbirth, nutrition, immunisation, the ‘milestones’ of physical development and measures of academic progress.
Provide accessible and relatable information to primary caregivers and all those raising under-fives to build their knowledge, emotional literacy and skills, so that they can engage in nurturing relationships and provide rich learning environments and experiences. The resources provided by the BBC’s Tiny Happy People are just one example, of many, of materials that are being created to help parents [103]. We need to think creatively and dynamically about how to make sure that information and knowledge about early childhood development reach all parents and wider society.
Educate the next generation. Changes in attitudes and behaviour will be achieved more quickly if knowledge is shared with school-age children, who in time will be the next generation of parents. Information about healthy brain development in the early years and the science that lies behind our understanding should be included in the school curriculum.
2. Building a mentally healthier and more nurturing society
Healthy development, from pregnancy onwards, requires nurturing relationships, environments and experiences. Everybody has a role to play, and collectively we have the power to:
Give greater priority to mental wellbeing across society, which in turn will better support parents and children, including by building greater emotional literacy to support social and emotional development in the early years.
Value the role of parents, carers and families, creating space for their voices to be heard. Listening is key to understanding needs and challenges and to identifying better ways to support healthy childhood development.
Invest in the mental health, wellbeing and emotional literacy of parents and caregivers to help build virtuous cycles of improved wellbeing and positive stable relationships across the lifespan. This includes ensuring that all health and social care professionals in contact with parents during pregnancy and in the early years have a sufficient understanding of parental mental health issues and of healthy parent-infant interactions and intergenerational trauma.
Build the capacity and capability of parents and caregivers to foster healthy relationships between adults and children, starting with strong bonds of attachment. This will support the foundations for mental wellbeing and resilience for the next generation. However, the feelings of judgement and isolation experienced by many parents point to a wider need to normalise and destigmatise the accessing of parenting support and programmes, in the same way that we have seen a destigmatisation of talking about mental health.
Address poverty. Parents can only engage with a system of support if they have the capacity to do so. Urgent steps are required to ensure that families with the youngest children are not struggling to survive without adequate nutrition, nappies and clothes and affordable and safe housing, and to ensure that the most vulnerable parents get the right specialist help in relation to mental health.
Create safe, healthy and nurturing environments and experiences, including rich home learning environments and high-quality early years education and childcare, and provide easy access to nature and outdoor space.
3. Creating communities of support
We can leverage human capital and connection so that families feel supported in all contexts. Other parents, the ecosystem of organisations that exist to support families in the early years and wider society all have a critical role to play. Non-parents have as important a role as parents in making communities family-friendly. Collectively we can:
Encourage and scale up parent-to-parent help. All parents and carers need support, with family and friends usually being the first port of call. There are wonderful examples of peer-support initiatives — from informal online groups to organised volunteer services — that help meet practical and emotional needs. In some places there are parent champions who are an invaluable and trusted source of information and who build bridges to local services.
Harness communities’ strengths in support of families. The pandemic, for all the challenges it has created, has served as a reminder of the power of community — from the explosion of mutual aid across the country to the more than a million people who signed up to volunteer with the NHS. Local charities and services have also worked together in new ways, gaining better understandings of families’ needs. Many families say that they feel better supported by their communities than in the past. Communities can build on this moment to:
Create welcoming, non-judgemental environments that support parental wellbeing, including outdoor and green spaces;
Encourage and support help-seeking, so that it is seen as the norm for parents to look for help and to receive it;
Use their voice to ensure that early childhood is prioritised.
Champion the value of high-quality, evidence-based parenting programmes and support. Parenting programmes have demonstrated the potential to prevent a range of social, emotional and behavioural problems. Evaluations have demonstrated that combined universal and targeted approaches reduce the prevalence of child and adult mental ill health and rates of child abuse and neglect.
In the workplace, encourage and facilitate a more family-friendly society. Our workplaces have huge power in shaping a culture that supports the early years, whether in terms of retaining staff or long-term investment in the development of a future productive workforce. In the US, 3,000 business leaders have signed up to ReadyNation, a movement that seeks to ‘strengthen business through smart investments in children and youth’ [104]. Many of those who are engaged have a wider perspective on the importance of the early years and are supporting early childhood programmes both within and outside of their own businesses. We need employers in the UK to do the same. Employers can support families in the early years by coming together to share ideas, experience and knowledge about supporting employees as they become parents, and for example by:
Supplementing statutory provision for paid leave, ensuring that all parents and carers have sufficient and equal paid maternity and paternity leave;
Providing flexibility in working hours to meet parents’ needs, and ensuring that they always have the confidence to ask for such arrangements. The pandemic has demonstrated that flexible working is possible, without damaging business, in many more jobs than we previously considered.
4. Strengthening the early years workforce
There are thousands of dedicated and hardworking individuals who are committed to supporting families in the early years, from pregnancy onwards. Their work is not always properly recognised or valued but, whether as midwives, health visitors, providers of early help and specialist support or early education and childcare workers, they make a huge difference. For example, it has been shown repeatedly that early childhood education and childcare can have a positive effect on children’s developmental outcomes when the quality of services is high [105]. Skilled and well-supported practitioners are key to the quality of services and can make a proven difference, particularly for children from low-income and at-risk families. We need to:
Recognise the importance of the role played by the early years workforce and reflect this in the quality of training, in support for workers’ emotional wellbeing and in the value we attach to their roles. Universal services and professionals (midwives and health visitors) and primary care services (GPs) must have the support and capacity to enable them to meet need and achieve a shift to both physical and mental health care.
Ensure that those who work with children and parents have good and easy access to the latest scientific research and support to translate the science into practice. Practitioner training needs to cover all aspects of healthy child development, including brain development and mental health guidance.
Encourage and enable practitioners to pull together, harnessing a sense of joint purpose and common cause in the early years sector. In some parts of the sector there is increasing understanding of the benefits of holistic training on all aspects of healthy childhood development. The Royal College of Midwives, for example, has published a guide on Parental Emotional Wellbeing and Infant Development, providing ‘focussed, clinically relevant and evidence based information and advice on the inextricably linked issues of parental mental health, the parent-baby relationship, and infant development’ [106].
5. Putting the data to work for early years
We can support research and put data more effectively to work for the early years. As already noted, data on babies and infants are both patchy and lacking in consolidation. At the same time, there are gaps in research — and where research does exist, it isn’t consistently used to inform practice. We need to:
Invest in research of all kinds to build our body of knowledge, including psychological, behavioural, social and implementation science, longitudinal studies and economic evaluations. A new study by the Centre for Longitudinal Studies (CLS), launched in May 2021 and tracking 8,000 families over their child’s first five years, is a great example of the kind of work we need to see more of [107].
Consistently use research and evidence to educate practice, and help commissioners of services and professionals to make the space to hear and effectively use that evidence.
Gather data routinely and consistently from birth onwards to allow for early identification of emotional and physical developmental needs and the tracking of outcomes. Robust datasets will also support research and so increase our knowledge of what makes a difference.
Harness knowledge from the private sector to find safe ways to share data between organisations. Data are vital to our understanding of need and outcomes, and rigorous collection of data and joining up of datasets (presently held in separate ‘silos’) are essential to forming a complete picture of the child.
6. Supporting long-term and intergenerational change
We can strengthen the foundations of support for all through making a long-term commitment to building and sustaining an effective system. This will require:
A national framework providing a common agenda to drive holistic and preventative early childhood support. We need continuity of care and a minimum level of support for the mental and physical wellbeing of all children and parents from pregnancy onwards. This should reflect what all parents need and value, and what evidence has shown will make a difference.
Deeper collaborative working at the local level. A new national framework will create more opportunities to develop shared priorities and deliver collective impact through the public, private and voluntary sectors working together more effectively. But collaboration also needs to be driven and owned locally by those working with families. There are some great examples of energy and effort being put into this way of thinking — for example, Early Learning Communities and the Team Around the Setting model. Children’s centres, family hubs and digital support all have a role to play. It will be essential to expand these kinds of approach and to harness new partnerships formulated in lockdown in order to provide families with more holistic support.
A measurable child outcomes framework that can be used throughout the early years and will help us to understand how children are developing at all ages and across all domains of development.
Conclusion
The more we learn about the first five years, the greater the imperative to act becomes. We must reframe the conversation so that this period of children’s lives is appreciated for the incredible opportunity that exists and so that nurturing this potential is seen as essential and not as merely ‘nice to have’. Anything less leaves us, as we have seen, playing catch-up, at significant human, economic and societal cost.
The time for action is now. The pandemic has provided a moment for reflection on the society that we can be. With a greater focus on early childhood, we have the opportunity to build a happier society and one that is mentally and physically healthier.
Nobody can pretend that this will be an ‘easy fix’. Identifying where to target preventative and early intervention work can in practice be hard. However, thanks to a huge and growing body of research from across disciplines, we know a great deal more now than at any point in the past about how to make a positive difference.
With this report, The Royal Foundation aims to raise awareness of the strategic importance of the early years and to drive action towards lasting change. To act, we will need to change the way we think about early childhood. We believe that everybody has a role to play in making this happen. Whether we are policy makers, early years practitioners, employers, neighbours, friends or wider family members of parents with young children, we can all support the development of nurturing relationships, positive environments and beneficial experiences in early childhood.
Together, we can provide the wider ecosystem of relationships and systems that help reduce adversity and promote healthy childhood development. This will ultimately benefit each and every one of us.
Endnotes
Vos, T. et al. (2013). Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study. The Lancet, 386 (9995). pp. 743-800.
Ipsos MORI. (2020). State of the Nation: Understanding Public Attitudes to the Early Years. The Royal Foundation. https://www.ipsos.com/sites/default/files/ipsos_public-attitudes-early-years-uk.pdf
Deacon, T.W. (2011). Incomplete Nature: How mind emerged from matter. New York: W.W. Norton.
Ipsos MORI. (2020). State of the Nation: Understanding Public Attitudes to the Early Years. The Royal Foundation. https://www.ipsos.com/sites/default/files/ipsos_public-attitudes-early-years-uk.pdf
Lenroot, R.K. & Giedd, J.N. (2006). Brain development in children and adolescents: insights from anatomical magnetic resonance imaging. Neuroscience & Biobehavioral Reviews, 30(6), 718-729.
The Center on the Developing Child at Harvard University. Brain Architecture. https://developingchild.harvard.edu/science/key-concepts/brain-architecture/
Shonkoff, J.P. & Phillips, D.A. (eds). (2000). From Neurons to Neighborhoods: The Science of Early Childhood Development. National Research Council (US) and Institute of Medicine (US) Committee on Integrating the Science of Early Childhood Development. https://pubmed.ncbi.nlm.nih.gov/25077268/
Hensch, T.K. (2005). Critical period plasticity in local cortical circuits. Nature Reviews Neuroscience. https://www.nature.com/articles/nrn1787
Holtmat, A. & Svoboda, K. (2009). Experience-dependent structural synaptic plasticity in the mammalian brain. Nature Reviews Neuroscience 10(9): 647-58. https://pubmed.ncbi.nlm.nih.gov/19693029/
Oberlander, T.F., Weinberg, J., Papsdorf, M., Grunau, R., Misri, S. & Devlin, A.M. (2008). Prenatal exposure to maternal depression, neonatal methylation of human glucocorticoid receptor gene (NR3C1) and infant cortisol stress responses. Epigenetics, 3; 97-106.
Links to the information and research studies are available at: https:// dunedinstudy.otago.ac.nz/
Moffitt, T.E., Arseneault, L., Belsky, D., Dickson, N., Hancox R.J. et al. (2011). A gradient of childhood self- control predicts health, wealth, and public safety. PNAS, 15 February 2011, 108(7), 2693-2698. https://doi.org/10.1073/pnas.1010076108
NHS Digital. (2018). Mental Health of Children and Young People in England 2017. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2017/2017
Shonkoff, J.P. & Garner, A.S. (2012). The Lifelong Effects of Early Childhood Adversity and Toxic Stress. The Committee on Psychosocial Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care, and Section on Developmental and Behavioral Pediatrics. Pediatrics, January 2012, 129(1) e232-e246. DOI: 10.1542/ peds.2011-2663
Gilbert, R., Wisdom, C.S., Browne, K., Fergusson, D., Webb, E. & Janson, S. (2009). Burden and consequences of child maltreatment in high-income countries. The Lancet, 373, 68-81. McCrory, E.J. & Viding, E. (2017).
McCrory, E.J. & Viding, E. (2017). Annual research review: childhood maltreatment, latent vulnerability and the shift to preventative psychiatry — the contribution of functional brain imaging. Journal of Child Psychology and Psychiatry and Allied Disciplines 58(4), 228-357.
Dawson, G., Frey, K., Panagiotides, H., Osterling, J. & Hessls, D. (1997). Infants of depressed mothers exhibit atypical frontal brain activity: A replication and extension of previous findings. Journal of Child Psychology and Psychiatry and Allied Disciplines 38(2), 179-186.
McCrory, E.J, De Brito, S.A., Sebastian, C.L., Mechelli, A., Bird, G., Kelly, P.A. & Viding, E. (2011). Heightened neural reactivity to threat in child victims of family violence. Current Biology, 21(23), R947-R948.
WHO. (2021). ICD-11 for Mortality and Morbidity Statistics (version 05/2021). https://icd.who.int/browse11/l-m/en#/
Hanlon, P., McCallum, M., Jani, B.D., McQueenie, R.D. & Mair, F.S. (2020). Association between childhood maltreatment and the prevalence and complexity of multimorbidity:
A cross-sectional analysis of 157,357 UK Biobank participants. Journal of Comorbidity, 10,1-12.Gerin, M.I., Viding, E., Pingault, J.B, Puetz, V.B., Knodt, A.R., Radtke, S.R. et al. (2019). Heightened amygdala reactivity and increased stress generation predict internalizing symptoms in adults following childhood maltreatment. Journal of Child Psychology and Psychiatry, 60(7), 752-761.
McCrory, E.J. (2020). ‘The case for a preventative approach to mental health: childhood maltreatment, neuroimaging, and the theory of latent vulnerability’, in Davies, W., Savulescu, J. & Roache, R. (eds). Psychiatry Reborn: Biopsychosocial Psychiatry in Modern Medicine. Oxford, UK: Oxford University Press.
National Scientific Council on the Developing Child. (2020). Connecting the Brain to the Rest of the Body: Early Childhood Development and Lifelong Health Are Deeply Intertwined. Working Paper No. 15. The Center on the Developing Child, Harvard University. https://46y5eh11fhgw3ve3ytpwxt9r-wpengine.netdna-ssl.com/wp-content/uploads/2020/06/wp15_health_FINALv2.pdf
Hackett, R.A. & Steptoe, A. (2017). Type 2 diabetes mellitus and psychological stress — a modifiable risk factor. Nature Reviews Endocrinology 13(9), 547-560.
Kullman, S., Heni, M., Hallschmid, M., Fritsche, A., Preissl, H. & Haring, H.U. (2016). Brain insulin resistance at the cross-roads of metabolic and cognitive disorders in humans. Physiological Reviews, 96(4), 1169-1209.
Dallman, M.F. (2010). Stress-induced obesity and the emotional nervous system. Trends in Endocrinology & Metabolism 21(3), 159-165.
The Center on the Developing Child, Harvard University. InBrief: The Impact of Early Adversity on Childhood Development. https://developingchild.harvard.edu/resources/inbrief-the-impact-of-early-adversity-on-childrens-development/
Bowlby, J. (1969). Attachment and Loss. Vol 1: Attachment. London, UK: Hogarth Press and Institute of Psychoanalysis.
National Scientific Council on the Developing Child. (2004). Young Children Develop in an Environment of Relationships: Working Paper No 1. The Center on the Developing Child, Harvard University. https://developingchild.harvard.edu/wp-content/uploads/2004/04/Young-Children-Develop-in-an-Environment-of-Relationships.pdf
Weintraub, S., Dikmen, S.S., Heaton, R.K., Tulsky, D.S., Zelazo, P.D. et al. (2014). NIH Toolbox for the Assessment of Behavioural and Neurological Function: Cognition domain instruments. Neurology.
Luyten, P., Campbell, C. & Fonagy, P. (2021). Rethinking the relationship between attachment and personality disorder. Current Opinion in Psychology, 37, 109-113. doi: 10.1016/j.copsyc.2020.11.003
Schweinhard, L.J. (2005). The High/Scope Perry Preschool study through age 40. https://highscope.org/wp-content/uploads/2018/11/perry-preschool-summary-40.pdf
Waldren, J. (2017). The Effective, Pre-School, Primary and Secondary Education project (EPPSE). Institute of Education, University College London. https://www.ucl.ac.uk/ioe/research-projects/2020/sep/effective-pre-school-primary-and-secondary-education-project-eppse
Ipsos MORI. (2020). State of the Nation: Understanding Public Attitudes to the Early Years. The Royal Foundation. https://www.ipsos.com/sites/default/files/ipsos_public-attitudes-early-years-uk.pdf
Links to the information and research studies are available at: https://dunedinstudy.otago.ac.nz/
Stansfeld, S., Clark, C., Bebbington, P., King, M., Jenkins, R. & Hinchliffe, S. (2016). ‘Chapter 2: Common mental disorders’. In McManus, S., Bebbington, P., Jenkins, R. & Brugha, T. (eds.). Mental Health and Wellbeing in England: Adult Psychiatric Morbidity Survey 2014. Leeds: NHS Digital. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/556596/apms-2014-full-rpt.pdf
NHS Digital. (2018). Mental Health of Children and Young People in England, 2017. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2017/2017
See Appendix 1 to Big Change Starts Small (2021). Technical report on Cost of Lost Opportunities in the early years 2018/2019. London School of Economics.
In 2016 the Early Intervention Foundation analysed the amount spent from the public purse in England and Wales on remedial action and interventions for older children and young adults. This analysis is not directly comparable with the LSE analysis, in that the LSE work focuses on England alone, excludes some of the EIF cost bases and includes other cost categories. https://www.eif.org.uk/report/the-cost-of-late-intervention-eif-analysis-2016
Based on spending cited in Britton, J., Farquharson, C., Sibieta, L., Tahi, I. & Waltmann, B. (2020). 2020 Annual Report on Education Spending in England. Institute for Fiscal Studies. https://ifs.org.uk/uploads/R182-2020-annual-report-on-education-spending-in-England.pdf
The Perinatal Mental Health Care Pathway (May 2018) NHS England, NHS Improvement, National Collaborating Centre for Mental Health. https://www.england.nhs.uk/wp-content/uploads/2018/05/perinatal-mental-health-care-pathway.pdf
NHS Mental Health Dashboard. https://www.england.nhs.uk/mental-health/taskforce/imp/mh-dashboard/. According to Department of Health and Social Care (DHSC) accounts and the NHS Mental Health Dashboard for Q4 2018/19, £12.5 billion was spent on mental health in that year. Of this, £10.6 billion was spent by Clinical Commissioning Groups (CCGs) on mental health and £1.9 billion on services commissioned by NHS England. These figures include £2.1 billion spent on dementia services and learning disabilities. Of the £12.5 billion, £7.5 billion is accounted for by the 2019 National Cost Collection, and it is a proportion of the £7.5 billion that has been included in the LSE analysis. NHS England and NHS Improvement. (2020). https://www.england.nhs.uk/wp-content/uploads/2020/08/1_-_NCC_Report_FINAL_002.pdf
Currie, J. & Spatz Widom, C. (2010). Long-term consequences of child abuse and neglect on adult economic well-being. Child Maltreatment, 15(2), 111-120
Cattan, S., Conti, G., Farquharson, C. & Ginja, R. (2019). The Health Effects of Sure Start. https://ifs.org.uk/publications/14139
See Appendix 2 to Big Change Starts Small (2021). Casestudies on the benefits of investment in the early years. London School of Economics.
Morrell, C.J. et al. (2016). A systematic review, evidence synthesis and meta-analysis of quantitative and qualitative studies evaluating the clinical effectiveness, the cost-effectiveness, safety and acceptability of interventions to prevent postnatal depression. Health Technology Assessment, 20(37): pp. 1-414.
Henderson, C. et al. (2019). Cost- effectiveness of PoNDER health visitor training for mothers at lower risk of depression: findings on prevention of postnatal depression from a cluster-randomised controlled trial. Psychological Medicine, 49(8): pp. 1324-1334.
Milgrom, J. et al. (2015). Feasibility study and pilot randomised trial of an antenatal depression treatment with infant follow-up. Archives of Women’s Mental Health, 18(5): pp. 717-730.
Stein, A. et al. (2018). Mitigating the effect of persistent postnatal depression on child outcomes through an intervention to treat depression and improve parenting: a randomised controlled trial. The Lancet Psychiatry, 5(2): pp. 134-144.
Petrou, S. et al. (2006). Cost- effectiveness of a preventive counseling and support package for postnatal depression. International Journal of Technology Assessment in Health Care, 22(4): pp. 443-53.
Heckman. The economics of human potential. https://heckmanequation.org/
García, J.L., Heckman, J.J., Leaf, D.E. & Prados, M.J. (2016). The Life- cycle Benefits of an Influential Early Childhood Program. IZA Institute of Labor Economics. http://ftp.iza.org/dp10456.pdf
Heckman, J. The Rate of Return to the HighScope Perry Preschool Program. https://www.nber.org/papers/w15471
Stanford, M. (2020). The seeds of success? Taking a closer look at new data on the impact of early childcare and education. Early Intervention Foundation blogpost, February 2020. https://www.eif.org.uk/blog/the-seeds-of-success-taking-a-closer-look-at-new-data-on-the-impact-of-early-childcare-and-education
World Health Organization. (2018). Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health and Human Potential. https://apps.who.int/iris/bitstream/handle/10665/272603/9789241514064-eng.pdf?sequence=1&isAllowed=y
Department for Education. (2019). Early Years Foundation Stage Profile Results in England, 2019. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/839934/EYFSP_2019_Main_Text_Oct.pdf
The Department for Education (DfE) defines a ‘good level of development’ as a child attaining at least the expected level of development across 12 of 17 early learning goals.
Hutchinson J. et al. (2020). Education in England: Annual Report 2020. Education Policy Institute. https://epi.org.uk/publications-and-research/education-in-england-annual-report-2020/
The Children’s Commissioner. (2021). Building Back Better. https://www.childrenscommissioner.gov.uk/report/building-back-better/
Kindred2 and YouGov. (2020). School Readiness. https://kindredsquared.org.uk/wp-content/uploads/2020/11/Kindred2-YouGov-School-Readiness.pdf
Bradbury, B., Corak, M., Waldfogel, J. & Washbrook, E. (2015). Too Many Children Left Behind: The US Achievement Gap in Comparative Perspective. New York: Russell Sage Foundation.
Von Klitzing, K., Dohnert, M., Kroll, M. & Grube, M. (2015). Mental disorders in early childhood. Deutsches Ärzteblatt International, 112(21-22):375-86. doi: 10.3238/ arztebl.2015.0375
Mental Health Of Children and Young People in England. (2017). Official Statistics. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2017/2017
NHS England. Perinatal Mental Health. https://www.england.nhs.uk/mental-health/perinatal/
Howard, L.M, Ryan, E.G., Trevillion, K. et al. (2018). Accuracy of the Whooley questions and the Edinburgh Postnatal Depression Scale in identifying depression and other mental disorders in early pregnancy. The British Journal of Psychiatry, 212(1), 50-56.
Cameron, E.E., Sedov, I.D. & Tomfohr- Madsen, L.M. (2016). Prevalence of paternal depression in pregnancy and postpartum: An updated meta-analysis. Journal of Affective Disorders, 206, 189-203.
Mencap. (2020). How common is learning disability? https://www.mencap.org.uk/learning-disability-explained/research-and-statistics/how-common-learning-disability
Public Health England. (2015). The determinants of health inequities experienced by children with learning disabilities. https://www.basw.co.uk/system/files/resources/basw_24424-2_0.pdf
The Children’s Commissioner. CHLDRN — Local and national data on childhood vulnerability. https://www.childrenscommissioner.gov.uk/chldrn/
Parker, S. (2021). It takes a village — how to make all childhoods matter. Little Village/ Joseph Rowntree Foundation. https://wp.littlevillagehq.org/wp-content/uploads/2021/02/Anniversary_1080px_V8.pdf
Eisenstadt, N. & Oppenheim, C. (2019). Parents, Poverty and the State: 20 Years of Evolving Family Policy. Policy Press.
Eisenstadt, N. & Oppenheim, C. (2019). Parents, Poverty and the State: 20 Years of Evolving Family Policy. Policy Press
Merz, E.C., Wiltshire, C.A. & Noble, K.G. (2019). Socioeconomic Inequality and the Developing Brain: Spotlight on Language and Executive Function. Child Development Perspectectives, 13(1):15-20. doi: 10.1111/cdep.12305
Public Health England. (2018). Health Profile for England: 2018. https://www.gov.uk/government/publications/health-profile-for-england-2018
Raleigh, V. & Holmes, J. (2021). The health of people from ethnic minority groups in England. The King’s Fund. https://www.kingsfund.org.uk/publications/health-people-ethnic-minority-groups-england#Maternal
Based on OECD data accessed in 2019 and summarised in Farquharson, C. (2019). Early Education and Childcare Spending. Institute for Fiscal Studies. https://ifs.org.uk/publications/14557
Jo Cox Commission on Loneliness. (2017). Combatting loneliness one conversation at a time: A call to action. https://d3n8a8pro7vhmx.cloudfront.net/jcf/pages/164/attachments/original/1620919309/rb_dec17_jocox_commission_finalreport.pdf?1620919309
Ipsos MORI. (2020). State of the Nation: Understanding Public Attitudes to The Early Years, p. 31. The Royal Foundation. https://www.ipsos.com/sites/default/files/ipsos_public-attitudes-early-years-uk.pdf
Ipsos MORI. (2020). State of the Nation: Understanding Public Attitudes to the Early Years, p. 12, p. 25.The Royal Foundation. https://www.ipsos.com/sites/default/files/ipsos_public-attitudes-early-years-uk.pdf
Joshi, P., Wallace, E. & Williams, L. (2015). Young children’s and families’ experiences of services aimed at reducing the impact of low-income: Participation work with children and families. London: Office of the Children’s Commissioner. https://core.ac.uk/download/pdf/74378962.pdf
Robb, Y., McInery, D. & Martin, C.J.H. (2013). Exploration of the experiences of young mothers seeking and accessing health services. Journal of Reproductive and Infant Psychology, 31(4):399-412. doi: 10.1080/02646838.2013.832181
McLeish, J. & Redshaw, M. (2017). Mothers’ accounts of the impact on emotional wellbeing of organised peer support in pregnancy and early parenthood: a qualitative study. BMC Pregnancy and Childbirth, 17(1):28. doi: 10.1186/s12884-017- 1220-0
Jeffery, D., Clement, S., Corker, E., Howard, L.M., Murray, J. & Thornicroft, G. (2013). Discrimination in relation to parenthood reported by community psychiatric service users in the UK: A framework analysis. BMC Psychiatry, 13(1):120. doi: 10.1186/1471-244X-13-120
NCT. (2017). The Hidden Half: Bringing postnatal mental illness out of hiding. https://www.nct.org.uk/sites/default/files/related_documents/NCT%20The%20Hidden%20Half_0.pdf
Teh, J.L., King, D., Watson, B. & Liu, S. (2014). Self-stigma, anticipated stigma, and help-seeking communication in people with mental illness. Portal, 11(1):1-18. doi: 10.5130/portal.v11i1.3295
Parental Emotional Wellbeing and Infant Development. (2019). The Royal Colleges of Midwives. https://www.rcm.org.uk/media/4645/parental-emotional-wellbeing-guide.pdf
Pascal, C., Bertram, T. & Cole- Alback, A. (2020). Early Years Workforce Review. Revisiting the Nutbrown Review — Policy and Impact. The Sutton Trust. https://www.suttontrust.com/wp-content/uploads/2020/08/Early-Years-Workforce-Review.pdf
Blanden, J. et al. (2020). Challenges for the childcare market: the implications of COVID-19 for childcare providers in England. Institute for Fiscal Studies. https://ifs.org.uk/publications/14990
Institute of Health Visiting. (2018). Written evidence from the Institute of Health Visiting to the parliamentary Health and Social Care Committee inquiry into the First 1000 Days of Life. London: Institute of Health Visiting. https://ihv.org.uk/news-and-views/news/ihv-publishes-submission-to-parliamentary-inquiry-into-the-first-1000-days-of-life/
Institute of Health Visiting. (2020). State of Health Visiting in England: Are babies and their families being adequately supported in England in 2020 to get the best start in life? http://allcatsrgrey.org.uk/wp/download/public_health/health_visiting/State-of-Health-Visiting-survey-2020-FINAL-VERSION-18.12.20.pdf
Office for National Statistics. (2021). Coronavirus and depression in adults, Great Britain: January to March 2021. https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/articles/coronavirusanddepressioninadultsgreatbritain/januarytomarch2021
Parent–Infant Foundation. (2020). Babies in Lockdown: Listening to parents to build back better. https://parentinfantfoundation.org.uk/our-work/campaigning/babies-in-lockdown/
Reed, J. & Parish, N. (2021). Working for Babies: Lockdown lessons from local systems. First 1001 Days Movement. https://parentinfantfoundation.org.uk/wp-content/uploads/2021/01/210121-F1001D_Working_for_Babies_v1.2-FINAL-compressed_2.pdf
Reed, J. & Parish, N. (2021). Working for Babies: Lockdown lessons from local systems. First 1001 Days Movement. https://parentinfantfoundation.org.uk/wp-content/uploads/2021/01/210121-F1001D_Working_for_Babies_v1.2-FINAL-compressed_2.pdf
Davies, C. & Hendry, A. (2021). Early childhood education and care (ECEC) during COVID-19 boosts growth in language and executive function. Infant and Child Development. https://doi.org/10.1002/icd.224
Ipsos MORI. (2020). State of the Nation: Understanding Public Attitudes to The Early Years, p. 44. The Royal Foundation. https://www.ipsos.com/sites/default/files/ipsos_public-attitudes-early-years-uk.pdf
Parker, S. (2021). It takes a village — how to make all childhoods matter. Little Village/ Joseph Rowntree Foundation. https://wp.littlevillagehq.org/wp-content/uploads/2021/02/Anniversary_1080px_V8.pdf
Royal College of Midwives. (2020). COVID-19 impact on Black, Asian and Minority ethnic (BAME) women. https://www.rcm.org.uk/media/4164/covid-19-impact-on-black-asian-and-minority-ethnic-bame-women.pdf
Children and Young People’s Commissioner Scotland. (2020). The pandemic’s impact on children and young people with disabilities and ASNs. https://cypcs.org.uk/coronavirus/independent-impact-assessment/pandemic-impact-children-young-people-disability-asn/
There was a 30% increase in the total number of notifications during the first six months of 2020–21 compared with the same period in 2019–20. There were 92 cases in April–September 2018, 78 cases in the same period in 2019, and 102 cases in 2020. Source: Department for Education. (2021). Serious incident notifications. https://explore-education-statistics.service.gov.uk/find-statistics/serious-incident-notifications
Bowyer-Crane, C. et al. (2021). The Impact of Covid-19 on School Starters: Interim briefing 1. Parent and school concerns about children starting school. Education Endowment Foundation. https://educationendowmentfoundation.org.uk/public/files/Impact_of_Covid19_on_School_Starters_-_Interim_Briefing_1_-_April_2021_-_Final.pdf
The Best Start for Life: A Vision for the first 1001 days. (2021). The Early Years Healthy Development Review. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/973112/The_best_start_for_life_a_vision_for_the_1_001_critical_days.pdf
BBC. Tiny Happy People. https://www.bbc.co.uk/tiny-happy-people
ReadyNation International is growing, and has 200 business leaders from outside the US signed up so far. See: https://www.readynationinternational.org/
McCoy, D.C., Yoshikawa, H., Ziol-Guest, K.M, Duncan, G.J., Schindler, H.S., Magnuson, K. et al. (2017). Impacts of Early Childhood Education on Medium and Long Term Educational Outcomes. Educational Researcher, 46(8), 474- 487. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6107077/
Royal College of Midwives. (2019). Parental Emotional Wellbeing and Infant Development. https://www.rcm.org.uk/media/4645/parental-emotional-wellbeing-guide.pdf
Centre for Longitudinal Studies. Children of the 2020s Study. https://cls.ucl.ac.uk/cls-studies/children-of-the-2020s-study/
Acknowledgements
The Royal Foundation, June 2021
This report was written by The Royal Foundation and is the product of rich collaboration with academics and practitioners from the UK and beyond.
We would like to thank The Center on the Developing Child at Harvard University for their expert guidance in the writing of this report. We are particularly grateful to James Cairns, Senior Director, Strategic Engagements and Organizational Learning, and Al Race, Deputy Director and Chief Knowledge Officer.
The Care Policy and Evaluation Centre (CPEC) at the London School of Economics and Political Science (LSE) undertook the analysis of the cost of lost opportunity and produced case studies for Appendix 2. The work was led by Dr Eva-Maria Bonin, Assistant Professorial Research Fellow at CPEC, with research assistance from Sheree Marshall, and it was supported by an external panel, including Dr Lynn Karoly, Dr Filipa Sampaio (Researcher in Health Economics, Uppsala University) and Tom McBride. The case studies in Appendix 2 were written by Annette Bauer, Research Fellow at CPEC, and Dr Madeleine Stevens, Assistant Professorial Research Fellow, also at CPEC.
The report could not have been written without the longstanding support, knowledge and expertise of the members of the Early Years Steering Group, formed by The Duchess of Cambridge. The Steering Group was chaired by Scott Greenhalgh and brought together David Holmes CBE, Kate Stanley, Naomi Eisenstadt CB, Professor Eamon McCrory, Dr Alain Gregoire, Professor Leon Feinstein, Annamarie Hassall MBE, Professor Jane Barlow, Professor Peter Fonagy OBE, Dr Matthew Patrick, Kate Billingham CBE and Ed Vainker.
Last, but not least, we are very grateful to Jodie Reed for her wisdom and guidance, and to David Wilson for copy-editing and to North for design and layout.
The Royal Foundation of The Duke and Duchess of Cambridge is a charity registered in England and Wales no. 1132048.
Appendices © LSE, 2021
All other text © The Royal Foundation, 2021

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.